Musculature of Upper Limb
The muscles of the upper limb are organized into specific compartments or regions: shoulder, arm, forearm, and hand. The muscles in these compartments commonly share similar neurovascular supply and overall function(s), with a few exceptions. The following section details the contents of each compartment.
A. Shoulder
The shoulder region is the most proximal portion of the upper extremity, serving as the connection between the upper limb and the trunk. It comprises a collection of joints organized in the shoulder girdle and is characterized by its ability to move through an extensive range of motion. The health and functionality of the shoulder complex often suffer as a result of the region's freedom of movement. Muscles of the shoulder complex include anterior and posterior axioappendicular muscles and intrinsic scapular muscles. The pectoral region makes up the anterior axioappendicular muscles, while superficial back muscles make up the posterior axioappendicular muscles. These two groups connect the upper limb (scapula, clavicle, and humerus) to the axial skeleton (vertebral column, sternum, and ribs). The axilla (armpit) is a pyramid-shaped space that is bound by the musculature and bones of this region. It contains important neurovascular structures that serve the upper limb.
Movements at the shoulder complex include elevation, depression, rotation, protraction and retraction of the scapula and flexion, extension, abduction, adduction, medial (internal) rotation, lateral (external) rotation, and circumduction of the humerus (arm), as shown in Figure 1.
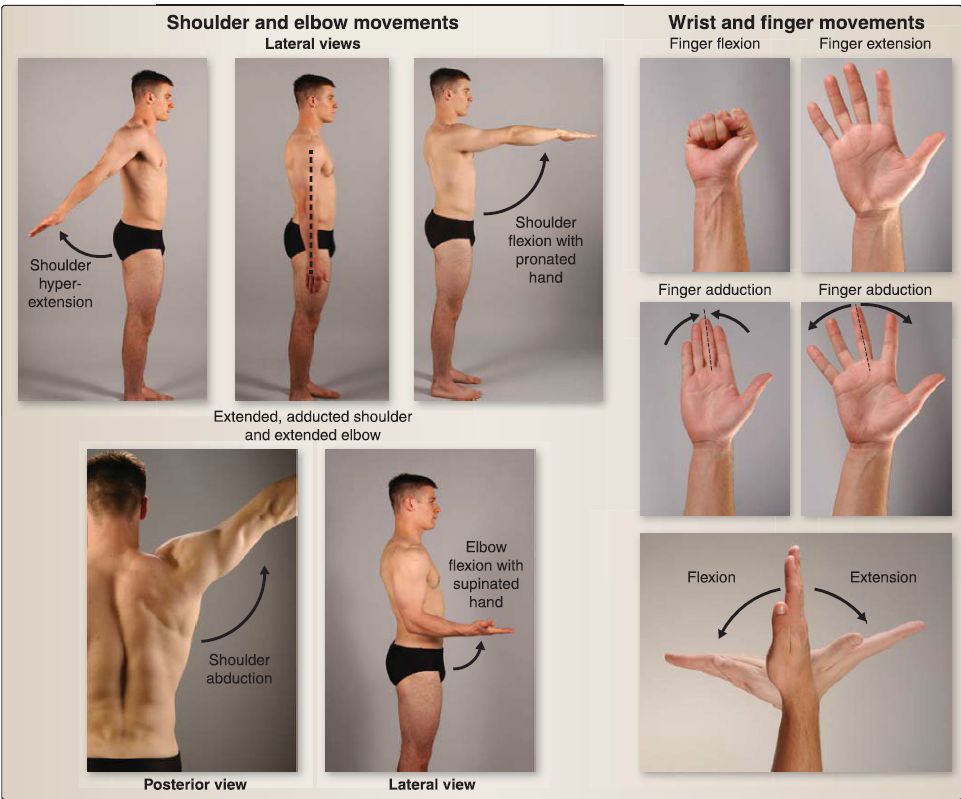 Figure 1: Movements of the upper limb joints.
Figure 1: Movements of the upper limb joints.
1. Anterior axioappendicular muscles: This group of muscles originates from the ribs, sternum, and clavicle to insert onto the humerus, scapula, and clavicle (Fig. 2).
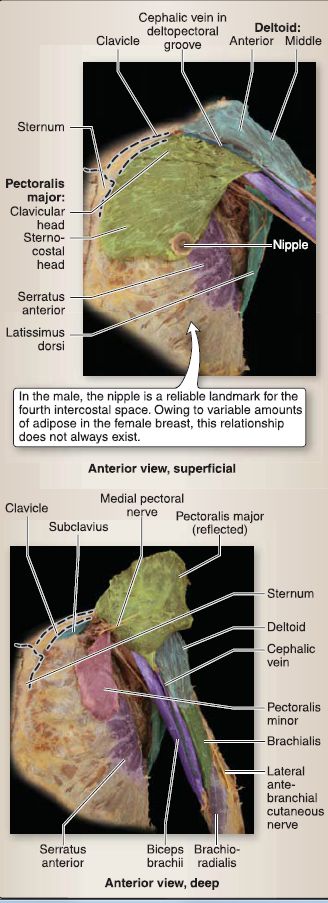
Figure 2: Anterior axioappendicular muscles.
a. Pectoralis major: This muscle has clavicular and sternocostal heads (origins) that collectively insert onto the lateral lip of intertubercular groove and adduct and medially rotate the arm.
[1] Clavicular head: This also flexes the arm and is innervated by the lateral pectoral nerve.
[2] Sternocostal head: This also extends arm from a flexed position and is innervated by the medial pectoral nerve.
b. Pectoralis minor: This muscle originates from ribs 3 to 5 to insert onto the coracoid process. It stabilizes the scapula by depressing and pulling anteriorly and is innervated by the medial pectoral nerve.
c. Serratus anterior: This muscle originates from ribs 1 to 8 and inserts onto the anterior medial border of the scapula. It protracts and rotates the scapula and stabilizes the scapula against the thoracic cage. It is innervated by the long thoracic nerve.
d. Subclavius: This muscle originates from the first rib and inserts onto the inferior clavicle. It anchors the clavicle and is innervated by the nerve to the subclavius.
2. Posterior axioappendicular muscles: This group of muscles originates from the axial skeleton (pelvis, spine, and occiput) and inserts onto the scapula, clavicle, and humerus (Fig. 3).
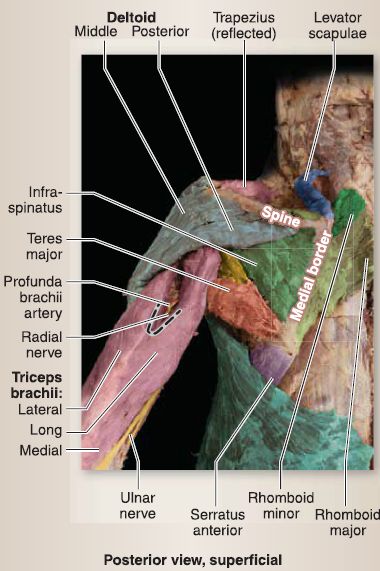

Figure 3:Posterior axioappendicular muscles.
a. Trapezius: This muscle originates from the external occipital protuberance, nuchal ligament, and thoracic spinous processes and inserts along the superior border of the scapular spine, acromion, and lateral third of the clavicle. It is innervated by the accessory nerve (cranial nerve XI) and has proprioceptive fibers from anterior rami C3--C4• This muscle has an upper, middle, and lower portion.
[1] Upper: This portion elevates and rotates the scapula upward.
[2] Middle: This portion retracts the scapula.
[3] Lower: This portion depresses and rotates the scapula upward.
b. Latissimus dorsi: This muscle originates from the iliac crest and thoracolumbar fascia and inserts into the floor of the intertubercular groove. It extends, adducts, and medially rotates the arm and is innervated by the thoracodorsal nerve.
c. Rhomboid major and minor: This pair of muscles originates from the inferior portions of the nuchal ligament (minor) and upper thoracic spinous processes (major) and inserts along the medial border of the scapula at the level of the spine (minor) and inferior (major). They retract and downwardly rotate the scapula and are innervated by the dorsal scapular nerve.
d. Levator scapulae: This muscle originates from cervical transverse processes and inserts along the superior medial border of the scapula. It elevates and downwardly rotates the scapula. Its upper slips are innervated by anterior rami C3-C4 and lower slips by the dorsal scapular nerve.
3. Intrinsic scapular muscles: Intrinsic scapular muscles arise directly from the scapula to insert onto the humerus (Fig. 4). This group includes the deltoid, teres major, supraspinatus, infraspinatus, teres minor, and subscapularis. The latter four comprise the rotator cuff muscles, which collectively work to stabilize the humeral head in the glenoid fossa and support the glenohumeral joint.
 Figure 4: Intrinsic scapular muscles.
Figure 4: Intrinsic scapular muscles.
a. Deltoid: This muscle originates along the inferior border of the scapular spine, acromion, and lateral third of the clavicle and inserts onto the deltoid tubercle. It is innervated by the axillary nerve. It is divided into anterior, middle, and posterior parts.
[1] Anterior: This part flexes and medially rotates the arm.
[2] Middle: This part is the main abductor of the arm.
[3] Posterior: This part extends and laterally rotates the arm.
b. Teres major: This muscle originates from the lateral border of the scapula and inserts onto the medial lip of the intertubercular groove. It adducts and medially rotates the arm and assists in arm extension. It is innervated by the lower subscapular nerve.
c. Supraspinatus: This muscle originates from the supraspinous fossa and inserts onto the (superior) greater tubercle. It initiates and assists in arm abduction and is innervated by the suprascapular nerve.
d. lnfraspinatus: This muscle originates from the infraspinous fossa and inserts onto the (middle) greater tubercle. It laterally rotates the arm and is innervated by the suprascapular nerve.
e. Teres minor: This muscle originates from the lateral border of the scapula and inserts onto the (inferior) greater tubercle. It laterally rotates the arm and is innervated by the axillary nerve.
f. Subscapularis: This muscle originates from the subscapular fossa and inserts onto the lesser tubercle. It adducts and medially rotates the arm and is innervated by the upper and lower subscapular nerves.
4. Axilla: The axilla is a pyramid-shaped space that spans between the root of the neck and arm (Fig. 5). It contains the infraclavicular portions of the brachia! plexus {chords and terminal branches), axillary vessels and branches, lymph vessels and nodes, and fat. Axillary vessels and nervous structures are contained within a fascial axillary sheath, which is continuous proximally with the cervical prevertebral fascia (Fig. 6).
a. Boundaries: The boundaries of the axil la are shown in Figure 5. [1] Anterior: This includes subclavius, pectoralis major and minor (anterior axillary fold) muscles, and overlying fascia.
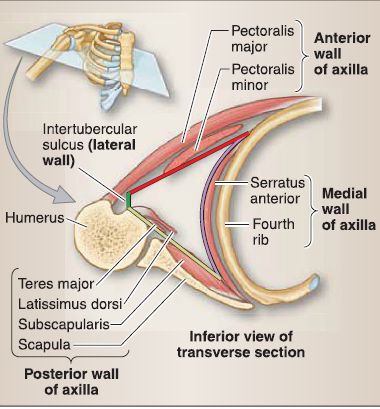
Figure 5: Axilla.
 Figure 6: Boundaries of axilla.
Figure 6: Boundaries of axilla.
[2] Posterior: This includes the scapula and subscapularis, latissimus dorsi, and teres major (posterior axillary fold) muscles.
[3] Medial: This includes the serratus anterior muscle and underlying ribs.
[4] Lateral: This includes the intertubercular groove of the humerus.
[5] Apex: This includes the superior border of the scapula, clavicle, and first rib (cervicoaxillary canal).
[6] Base: This includes skin and axillary fascia.
b. Blood supply: The shoulder complex is supplied mainly by branches from the axillary artery . Posterior axioappendicular and intrinsic scapular muscles also receive vasculature from subclavian artery branches (suprascapular, dorsal scapular, and transverse cervical).
5. Innervation: Cutaneous innervation of the shoulder region is mediated by superior lateral brachia! cutaneous (from axillary) supraclavicular and intercostobrachial nerves . The skin overlying the superficial back muscles (posterior axioappendicular group) is segmentally innervated by posterior primary rami. The main dermatomes in the shoulder region are C4-C6 and T2-T4 .
B. Arm
The humerus is the main bone of the arm, which spans between the shoulder (glenohumeral) and elbow (humeroradial, humeroulnar, and proximal radioulnar) joints. Brachia! fascia divides the arm into anterior and posterior compartments. Muscles of the arm cross both the shoulder and elbow joints; thus, some act at both joints. Muscles of the arm flex and extend the arm and flex, extend, and supinate the forearm.
1. Anterior arm: These muscles are primarily flexors of the forearm, but can also flex the arm. All anterior compartment muscles are innervated by the musculocutaneous nerve (C5-C7). Branches from the brachia! artery serve this compartment. Anterior arm muscles are shown in Figures 7and 8.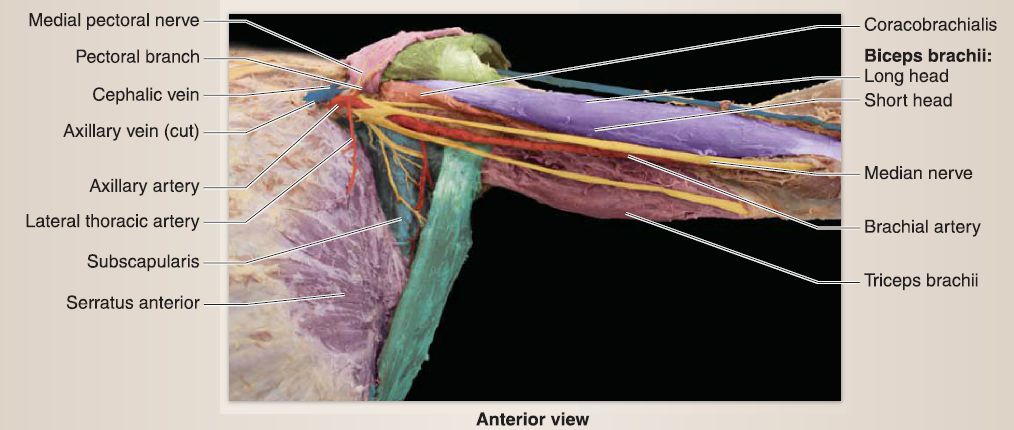
Figure 7:Superficial arm structures.
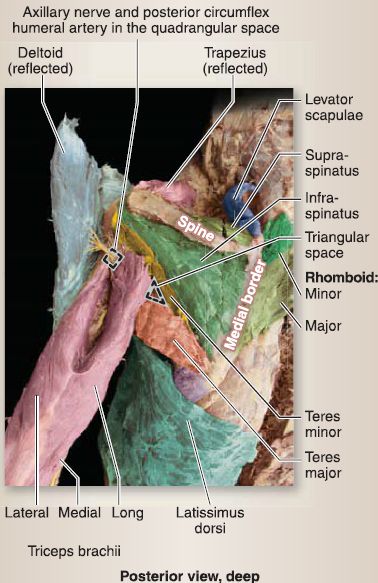
Figure 8: Deep anterior arm structures.
Biceps brachii: This two-headed muscle (short and long heads) originates from the supraglenoid tubercle (long) and coracoid process (short) and inserts through a common tendon on the radial tuberosity and antebrachial fascia by way of the bicipital
aponeurosis. It flexes the arm, supinates the forearm and flexes the forearm when it is supinated, and resists anterior glenohumeral dislocation.
b. Coracobrachialis: This muscle originates on the coracoid process and inserts along the medial midshaft of humerus. It assists in flexion and adduction of arm and resists anterior glenohumeral dislocation.
c. Brachialis: This muscle originates on the distal half of the anterior humerus and inserts onto the coronoid process and tuberosity of ulna. It is the primary flexor of the forearm (any position).
2. Posterior arm: These muscles are primarily extensors of the forearm, but can also extend the arm. All posterior compartment muscles are innervated by the radial nerve (C5-C8, T1). Branches from the profunda brachii artery serve this compartment. Posterior arm muscles are shown in Figure 9.
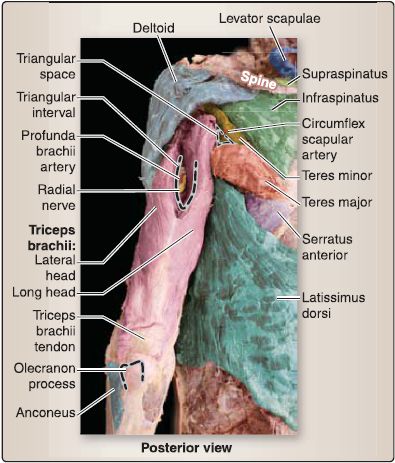
Figure 9: Posterior arm structures.
a. Triceps brachii: This three-headed muscle (long, lateral, and medial heads) originates from the infraglenoid tubercle (long), lateral to the radial groove (lateral), and medial to the radial groove (medial) and inserts through a common tendon on the olecranon process and antebrachial fascia. It extends the arm (long head) and the forearm.
b. Anconeus: This muscle originates from the lateral epicondyle of the humerus and inserts onto the olecranon and posterior proximal ulna. It assists in terminal extension of the arm and stabilizes the elbow.
3. Innervation: Cutaneous innervation of the arm is mediated primarily by inferior lateral brachia! cutaneous (from radial), medial brachial cutaneous, and posterior brachia! cutaneous (from radial) nerves . The main dermatomes in the arm are C8-C6 and T1-T2 .
C. Forearm
The radius and ulna make up the bones of the forearm, which spans between the elbow and wrist. Antebrachial fascia divides the forearm into anterior and posterior compartments. Muscles of the forearm cross the elbow, wrist, and hand joints; thus, some act at more than one joint. Muscles of the forearm flex, extend, pronate, and supinate the forearm; flex, extend, abduct (radial deviation), and adduct (ulnar deviation) the hand; and assist inflexion and extension of digits two through five and
flexion, extension, and abduction of the first digit (thumb).
1. Anterior forearm: Anterior forearm muscles are primarily flexors of the hand and digits, but can also assist inflexion and pronation of the forearm. Anterior compartment muscles are primarily innervated by the median nerve (C5-C8, T1). The ulnar nerve (C8-T1) innervates one and a half anterior forearm muscles. Branches from the radial and ulnar arteries serve this compartment. Anterior forearm muscles are divided into superficial, intermediate, and deep groups (Fig. 10).
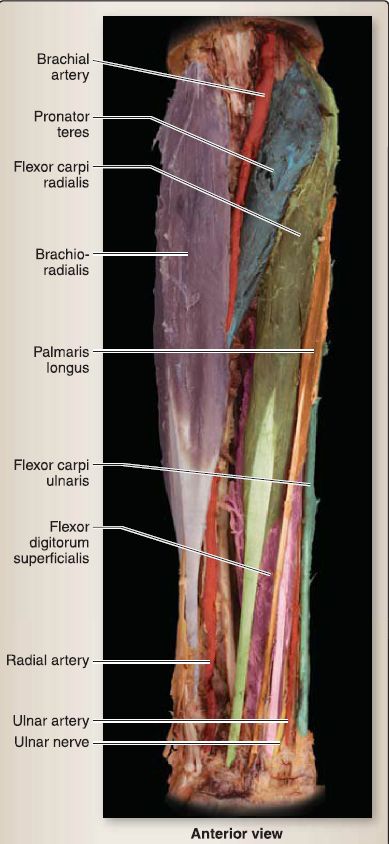
Figure 10 : Flexor forearm structures. Superficial and intermediate layers.
a. Superficial: The common flexor tendon serves as the collective origin for most muscles in this group.
[1] Pronator teres: This muscle originates from the medial epicondyle of the humerus and the coronoid process of the ulna and inserts onto the midshaft lateral radius. It pronates and flexes the forearm and is innervated by the median nerve.
[2] Flexor carpi radialis: This muscle originates from the medial epicondyle of the humerus and inserts onto the second metacarpal base. It flexes and abducts the hand and is innervated by the median nerve.
[3] Palmaris longus: This muscle, when present, originates from the medial epicondyle of the humerus and inserts into the palmar aponeurosis. It flexes the hand and puts tension on the palmar aponeurosis. It is innervated by the median nerve.
[4] Flexor carpi ulnaris: This muscle originates from the olecranon and inserts onto the carpal (pisiform and hamate) and fifth metacarpal bones. It flexes and adducts the hand and is innervated by the ulnar nerve.
b. Intermediate: The flexor digitorum superficialis is the muscle that originates from the medial epicondyle of the humerus, coronoid process of the ulna, and the proximal radius and inserts onto the shafts of the middle phalanges of digits two through five (see Fig. 10). It assists in hand flexion and flexes the second through fifth proximal interphalangeal (PIP) and metacarpophalangeal (MCP) joints. It is innervated by the median nerve.
c. Deep: Figure 11 shows muscles in this group. [1] Flexor digitorum profundus: This muscle originates from the proximal ulna and interosseous membrane and inserts onto the base of distal phalanges of digits two through five. It assists in hand flexion and flexes the second through fifth distal interphalangeal (DIP) joints. Its lateral half is innervated by the anterior interosseous nerve (deep branch of median nerve). Its medial half is innervated by the ulnar nerve.
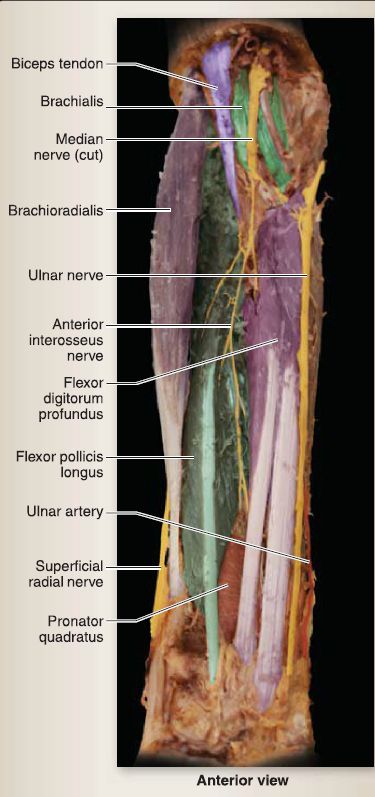
Figure 11: Flexor forearm structures. Deep layer.
[2] Flexor pollicis longus: This muscle originates from the middle radius and interosseous membrane and inserts onto the base of the distal phalanx of the thumb. It flexes the interphalangeal (IP) joint of the thumb and is innervated by the anterior interosseous nerve.
[3] Pronator quadratus: This muscle originates on the distal ulna and inserts onto the distal radius. It pronates the forearm and supports the distal radioulnar joint. It is innervated by the anterior interosseous nerve.
2. Posterior forearm: Posterior forearm muscles are primarily extensors of the hand and digits, but can also assist in flexion and supination of the forearm (Fig. 12).

Figure 13: Extensor forearm structures. Superficial layer.
Posterior compartment muscles are innervated by the radial nerve (C5-C8, T1) and its branches (Figs. 14 and 15). Branches from the radial and ulnar arteries serve this compartment. Posterior forearm muscles are divided into superficial and deep groups.
a. Superficial: The common extensor tendon serves as the collective origin for a portion of this group.
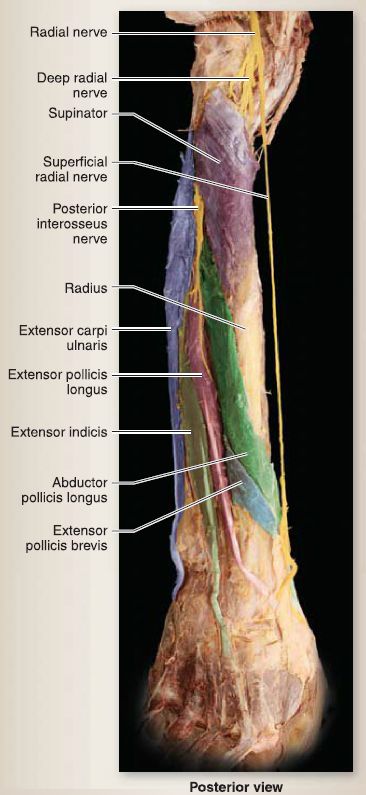
Figure 14: Extensor forearm structures. Deep layer
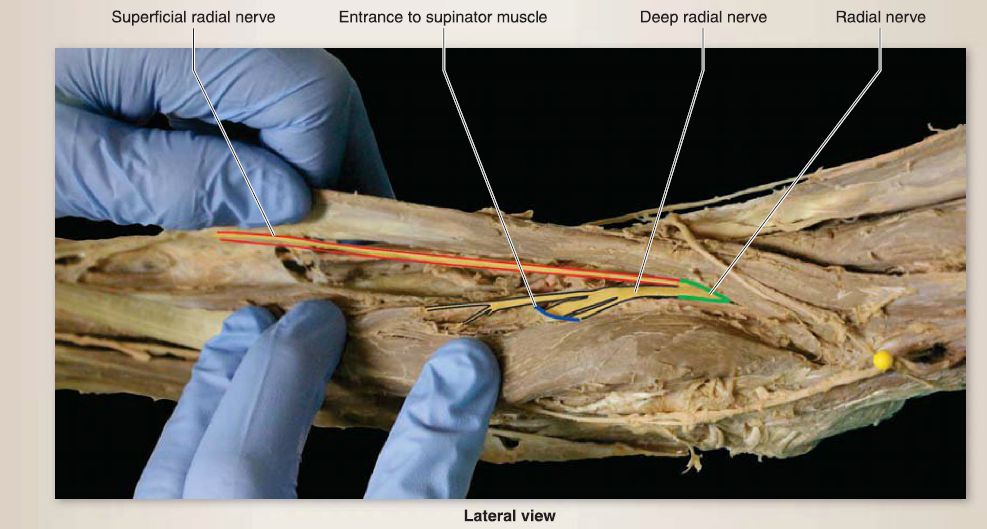 Figure 15 : Branching of radial nerve at elbow.
Figure 15 : Branching of radial nerve at elbow.
[1] Brachioradialis: This muscle originates from the supraepicondylar ridge of the humerus and inserts onto the distal lateral radius. It assists inflexion of the forearm (when in the midpronated position) and is innervated by the radial nerve.
[2] Extensor carpi radialis longus: This muscle originates from the lateral supraepicondylar ridge of the humerus and inserts onto the second metacarpal base. It extends and abducts the hand and is innervated by the radial nerve.
[3] Extensor carpi radialis brevis: This muscle originates from the lateral epicondyle of the humerus and inserts onto the third metacarpal base. It extends and abducts the hand and is innervated by the deep radial nerve.
[4] Extensor digitorum: This muscle originates from the lateral epicondyle of the humerus and inserts onto the extensor expansions of digits two through five. It extends digits two through five at MCP joints and assists in IP extension. It is innervated by the posterior interosseous nerve.
[5] Extensor digiti minimi: This muscle originates from the lateral epicondyle of the humerus and inserts onto the extensor expansion of the fifth digit. It extends the fifth digit at MCP joints and assists in IP extension. It is innervated by the posterior interosseous nerve.
[6] Extensor carpi ulnaris: This muscle originates from the lateral epicondyle of the humerus and posterior ulna and inserts onto the dorsal base of the fifth metacarpal. It extends and adducts the hand and is innervated by the posterior interosseous nerve.
b. Deep: Figure 16 shows muscles in this group.
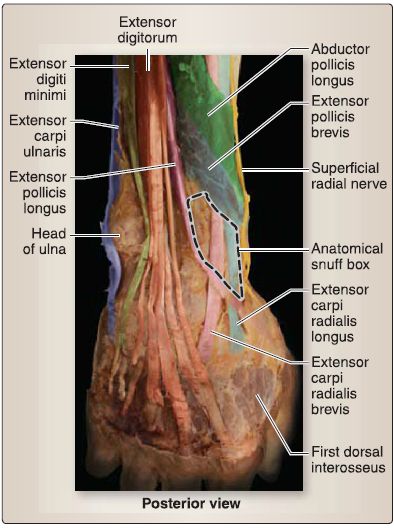
Figure 16 : Anatomical snuffbox and dorsum of hand.
[1] Supinator: This muscle originates from the lateral epicondyle of the humerus, radial ligaments, ulnar crest, and supinator fossa. It supinates the forearm and is innervated by the deep radial nerve.
[2] Outcropping muscles: All outcropping muscles in the deep compartment are innervated by the posterior interosseous nerve.
a. Abductor pollicis long us: This muscle originates from the proximal ulna, radius, and interosseous membrane and inserts onto the base of the first metacarpal bone.
It abducts the thumb and aids in extension at the carpometacarpal (CMG) joint.
b. Extensor pollicis longus: This muscle originates from the midshaft of the ulna and interosseous membrane and inserts onto the base of the distal phalanx of the thumb.
It extends all thumb joints.
c. Extensor pollicis brevis: This muscle originates from the distal radius and interosseous membrane and inserts onto the base of the proximal phalanx of the thumb. It extends the MCP and CMG joints.
d. Extensor indicis: This muscle originates from the distal ulna and interosseous membrane and inserts onto the extensor expansion of the second digit. It extends the second digit (allows for extension independent of other digits) and assists in wrist extension.
3. Cubital fossa: The cubital fossa is a triangular-shaped region on the anterior elbow surface (Fig. 17). It is bound medially by the pronator teres, laterally by the brachioradialis, and superiorly by an imaginary line through the medial and lateral epicondyles of the humerus. The floor of the fossa is made up of the supinator and brachialis muscles, and the roof is the overlying fascia, adipose, and skin. Important neurovascular structures course within and superficial to the fossa, and their anatomical relationships are important to understand because the cubital fossa is a common area for drawing blood samples.
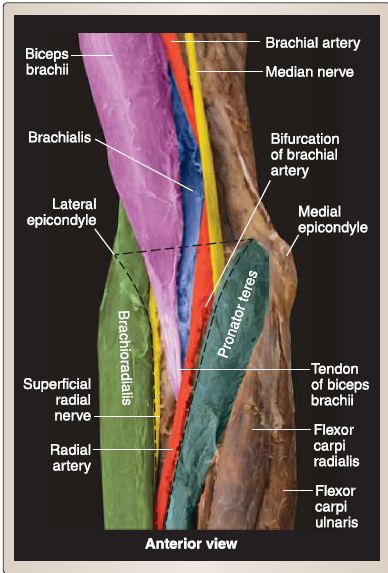
Figure 17: Cubital fossa. Black dotted line marks cubital fossa boundaries.
a. Contents: From lateral to medial, the contents are radial nerve and divisions (deep and superficial radial nerves), biceps brachii tendon, terminal portion of the brachia! artery as it branches into radial and ulnar arteries (with accompanying deep veins), and the median nerve.
b. Innervation: Superficially, the median cubital vein courses across the cubital fossa, connecting cephalic and basilic veins. Medial and lateral antebrachial cutaneous nerves travel superficially alongside the basilic and cephalic veins, respectively.
4. Innervation: Cutaneous innervation of the forearm is mediated primarily by lateral antebrachial cutaneous (from musculocutaneous), medial antebrachial cutaneous, and posterior antebrachial cutaneous (from radial) nerves . The main dermatomes in the arm are C5-C8 and T1 .
D. Hand
The hand is the distalmost portion of the upper limb and is connected to the forearm at the wrist. The hand is made up of 2 rows of carpal bones, 5 metacarpals, and a total of 14 phalangeal bones. The hand can be separated into three compartments, the thenar eminence (first digit muscular mass), hypothenar eminence (fifth digit muscular
mass), and a central compartment. The deep fascia of the handpalmar aponeurosis-covers the central compartment and further separates it from the thenar and hypothenar eminences. Terminal branches of the radial and ulnar arteries anastomose in a series of arterial arches to supply the hand. Hand movements include flexion, extension, abduction, and adduction of the digits as well as opposition of the first and fifth digits (Fig. 18). The third digit represents the midline of the hand.
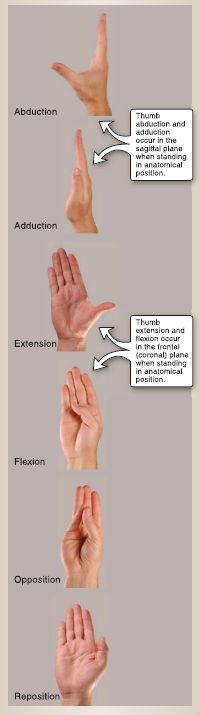
Figure 18: Movements of the thumb (first digit).
1. Thenar compartment: The thenar eminence is the muscular mass associated with the first digit-the thumb. Muscles in this compartment are innervated by the recurrent branch of the median nerve and include the abductor pollicis brevis, flexor pollicis brevis, and opponens pollicis (Fig. 19). Although not directly in the thenar eminence, the adductor pollicis does contribute to thumb movement. It is innervated by the deep branch of the ulnar nerve. Movement of the thumb is complex and imparts precision with fine motor tasks. At the CMC joint, abduction and adduction occur out of the palm in the sagittal plane, while flexion and extension occur in the frontal plane. Opposition is a complex motion that combines CMC extension, abduction, and medial rotation with MCP flexion.Flexor pollicis longus, abductor pollicis longus, extensor pollicis longus, and extensor pollicis brevis assist the intrinsic thumb muscles in achieving these movements.
 Figure 19: Superficial palmar hand.
Figure 19: Superficial palmar hand.
2. Hypothenar compartment: The hypothenar eminence is the muscular mass associated with the fifth digit-the little finger. Muscles in this compartment are innervated by the deep branch of the ulnar nerve and include the abductor digiti minimi, flexor digiti minimi brevis, and opponens digiti minimi (Fig. 20). Palmaris brevis overlies the hypothenar group and shares a common innervation. It is located superficially to the hypothenar eminence and aids in increasing grip by wrinkling the skin on the medial palm.
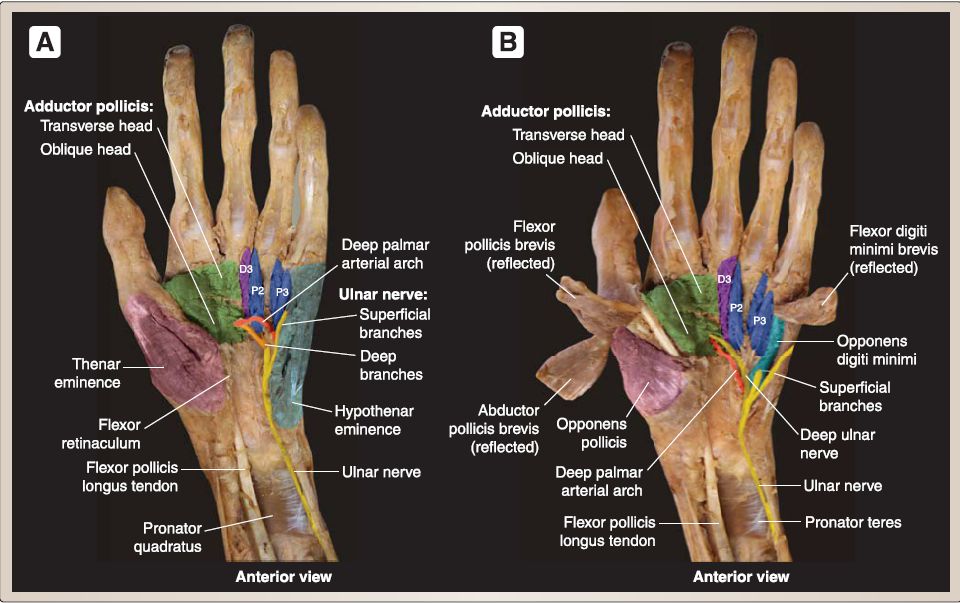 Figure 20 :Deep palmar hand. A, Thenar and hypothenar eminences intact. B, Thenar and hypothenar eminences reflected to show deeper structures. D - dorsal, P - palmar
Figure 20 :Deep palmar hand. A, Thenar and hypothenar eminences intact. B, Thenar and hypothenar eminences reflected to show deeper structures. D - dorsal, P - palmar
3. Central compartment: The central compartment of the hand contains tendons of the long flexors and short intrinsic hand muscles-four lumbricals and seven interossei (three palmar and four dorsal). The lateral two lumbricals are innervated by the median nerve, while the remaining central compartment muscles are innervated by the deep
branch of the ulnar nerve (see Figs. 19 and 20A). Lumbricals arise from the tendons of the flexor digitorum profundus and insert into the lateral extensor expansions of digits two through five (see Fig. 20 B). They flex the MCP joints and extend the IP joints of these digits. Dorsal interossei are bipennate muscles found between the metacarpals. Dorsal interossei abduct digits two through four. Palmar interossei are also found between metacarpals and adduct digits two, four, and five.
4. Carpal tunnel: The carpal tunnel is an osseofascial space that is bound posterolaterally by carpal bones and anteriorly by the thickened flexor retinaculum. The space is occupied by the median nerve and long tendons of flexor digitorum superficialis (4), flexor digitorum profundus (4), and flexor pollicis longus (1). Prior to entering the carpal tunnel, the median nerve gives off a cutaneous branch to the skin of the lateral palm-palmar cutaneous branch of the median nerve. After passing through the carpal tunnel, the median nerve divides into three to four palmar digital nerves and the recurrent branch of the median nerve to serve the thenar muscles; lumbricals (1 and 2); and the skin overlying digits one, two, three, and half of four. Compromise of the median nerve within the carpal tunnel may cause downstream motor and sensory impairments.
5. Innervation: Cutaneous innervation of the hand is mediated through branches of the ulnar, median, and radial nerves (Fig. 21). The median nerve innervates the skin over the lateral palm; thumb; and digits two, three, and half of four (extending to dorsum of the fingers to the DIP joint). The ulnar nerve innervates the skin over the medial palm and dorsum of the hand and digits five and half of four. The superficial radial nerve serves the lateral dorsum of the hand up to the PIP joints of digits two, three, and half of four. Dermatomes of the hand include C6 (thumb), C7 (digits two and three), and C8 .

Figure 21: Cutaneous and dermatome map of the hand. Cutaneous map of palm and dorsum of hand. Green region is supplied by the median nerve, yellow region is supplied by the radial nerve (superficial branch), and blue region is supplied by the ulnar nerve.





















