























النبات

مواضيع عامة في علم النبات
الجذور - السيقان - الأوراق
النباتات الوعائية واللاوعائية
البذور (مغطاة البذور - عاريات البذور)
الطحالب
النباتات الطبية
الحيوان
مواضيع عامة في علم الحيوان
علم التشريح
التنوع الإحيائي
البايلوجيا الخلوية
الأحياء المجهرية
البكتيريا
الفطريات
الطفيليات
الفايروسات
علم الأمراض
الاورام
الامراض الوراثية
الامراض المناعية
الامراض المدارية
اضطرابات الدورة الدموية
مواضيع عامة في علم الامراض
الحشرات
التقانة الإحيائية
مواضيع عامة في التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحيوية والميكروبات
الفعاليات الحيوية
وراثة الاحياء المجهرية
تصنيف الاحياء المجهرية
الاحياء المجهرية في الطبيعة
أيض الاجهاد
التقنية الحيوية والبيئة
التقنية الحيوية والطب
التقنية الحيوية والزراعة
التقنية الحيوية والصناعة
التقنية الحيوية والطاقة
البحار والطحالب الصغيرة
عزل البروتين
هندسة الجينات
التقنية الحياتية النانوية
مفاهيم التقنية الحيوية النانوية
التراكيب النانوية والمجاهر المستخدمة في رؤيتها
تصنيع وتخليق المواد النانوية
تطبيقات التقنية النانوية والحيوية النانوية
الرقائق والمتحسسات الحيوية
المصفوفات المجهرية وحاسوب الدنا
اللقاحات
البيئة والتلوث
علم الأجنة
اعضاء التكاثر وتشكل الاعراس
الاخصاب
التشطر
العصيبة وتشكل الجسيدات
تشكل اللواحق الجنينية
تكون المعيدة وظهور الطبقات الجنينية
مقدمة لعلم الاجنة
الأحياء الجزيئي
مواضيع عامة في الاحياء الجزيئي
علم وظائف الأعضاء
الغدد
مواضيع عامة في الغدد
الغدد الصم و هرموناتها
الجسم تحت السريري
الغدة النخامية
الغدة الكظرية
الغدة التناسلية
الغدة الدرقية والجار الدرقية
الغدة البنكرياسية
الغدة الصنوبرية
مواضيع عامة في علم وظائف الاعضاء
الخلية الحيوانية
الجهاز العصبي
أعضاء الحس
الجهاز العضلي
السوائل الجسمية
الجهاز الدوري والليمف
الجهاز التنفسي
الجهاز الهضمي
الجهاز البولي
المضادات الميكروبية
مواضيع عامة في المضادات الميكروبية
مضادات البكتيريا
مضادات الفطريات
مضادات الطفيليات
مضادات الفايروسات
علم الخلية
الوراثة
الأحياء العامة
المناعة
التحليلات المرضية
الكيمياء الحيوية
مواضيع متنوعة أخرى
الانزيمات

Cancer of unknown primary (CUP)
 المؤلف:
Stuart H. Ralston , Ian D Penman, Mark W J Strachan , Richard Hobson
المؤلف:
Stuart H. Ralston , Ian D Penman, Mark W J Strachan , Richard Hobson
 المصدر:
Davidsons Principles and Practice of Medicine
المصدر:
Davidsons Principles and Practice of Medicine
 الجزء والصفحة:
24th E , p138-139
الجزء والصفحة:
24th E , p138-139
 2025-02-04
2025-02-04
 1057
1057




+
-
20
When a patient is found to have advanced or metastatic cancer but history, examination and imaging is unable to define a primary cancer site, an assessment of patient fitness, disease extent, comorbidities and patient wishes should be made. Selected investigations should be carried out (Box1). However, a primary cancer site does not need to be ‘hunted down’ in all patients and investigations should be limited to those that will help management. Specialist investigations (e.g. endos copies) are only indicated when there is radiological suspicion or if there are localising symptoms.
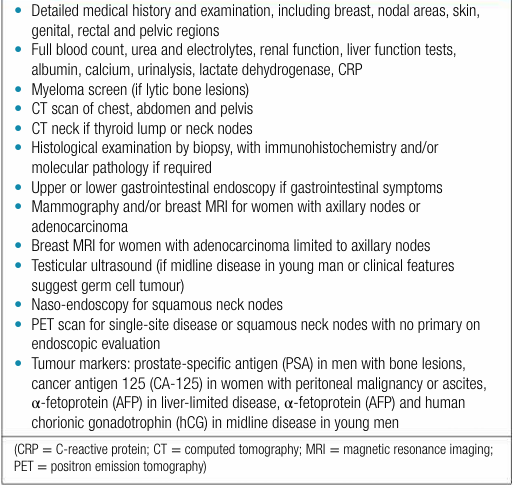
Box1. Initial diagnostic tests in patients presenting with carcinoma of unknown primary
In some cases, such as those with clinical suspicion of germ cell tumours, high-grade lymphoma or small cell cancer, or those presenting with oncological emergencies, urgent referral directly to oncology or haematology is essential to allow rapid initiation of anti-cancer therapy, sometimes before investigations are completed (Fig. 1).

fig1. Young male patient presenting with a bulky midline tumour and elevated HCG and AFP suggestive of a non-seminomatous testicular cancer.
If patients are fit to undergo investigations and fit enough to be considered for treatment then a core biopsy of the most accessible metastatic lesion is usually the quickest way of obtaining tissue for pathological evaluation of cancer type. Review of tumour morphology, immunohistochemistry and molecular pathology will usually be sufficient to plan appropriate treatment. Patients with clinicopathological features suggestive of a particular cancer should be identified early and referred promptly to the appropriate multidisciplinary/oncology team for consideration of further investigations and treatment. Where the primary site remains unclear following comprehensive investigations, a patient is said to have a cancer of unknown primary (CUP).
Whilst it is crucial to identify patients with highly treatable CUPs (Box2), some of whom can live for years , or even be cured by treatment, most CUPs are poorly differentiated cancers or adenocarcinomas with liver and/or multi-site metastases. These cancers often behave aggressively so early discussion with oncology, within the context of a specialist MDT, is essential to streamline investigations and assess fitness for anti-cancer treatment. Whilst responses to generic systemic anti-cancer treatment are modest, gene expression tests or molecular tumour profiling are increasingly providing greater information about likely tissue of origin or possible treatment targets which may ultimately lead to improved understanding of CUP and better outcomes.
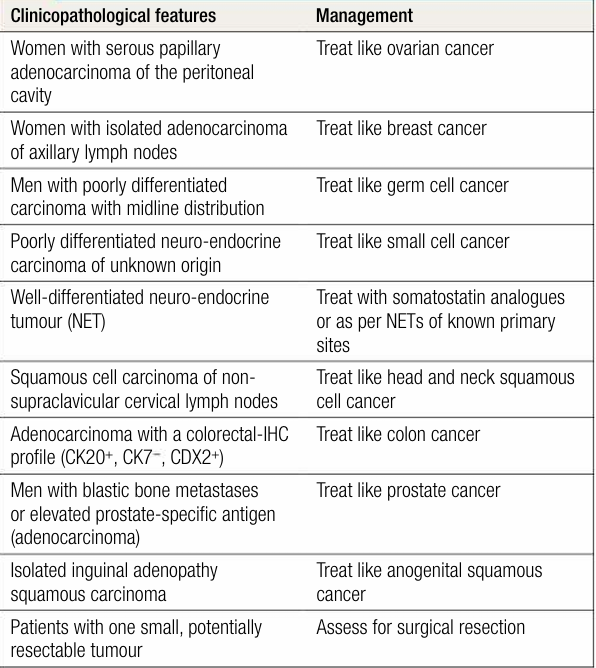
Box2. Cancer of unknown primary – favourable clinicopathological features.
 الاكثر قراءة في الاورام
الاكثر قراءة في الاورام
 اخر الاخبار
اخر الاخبار
اخبار العتبة العباسية المقدسة

الآخبار الصحية


مواضيع ذات صلة
 قسم الشؤون الفكرية يصدر كتاباً يوثق تاريخ السدانة في العتبة العباسية المقدسة
قسم الشؤون الفكرية يصدر كتاباً يوثق تاريخ السدانة في العتبة العباسية المقدسة "المهمة".. إصدار قصصي يوثّق القصص الفائزة في مسابقة فتوى الدفاع المقدسة للقصة القصيرة
"المهمة".. إصدار قصصي يوثّق القصص الفائزة في مسابقة فتوى الدفاع المقدسة للقصة القصيرة (نوافذ).. إصدار أدبي يوثق القصص الفائزة في مسابقة الإمام العسكري (عليه السلام)
(نوافذ).. إصدار أدبي يوثق القصص الفائزة في مسابقة الإمام العسكري (عليه السلام)



















