Malaria is an acute infectious disease of the blood, caused by one of five species of the protozoal genus, Plasmodium, which is a sporozoan. P. falciparum accounts for some 15 percent of all malaria cases, and P. vivax for 80 percent of malarial cases. The plasmodial parasite is transmitted to humans through the bite of a female Anopheles mosquito or by an infected, blood-contaminated, needle. Sporozoans reproduce asexually in human cells by a process called schizogony, in which multiple nuclear divisions are followed by envelopment of the nuclei by cell walls producing merozoites. These, in turn, become trophozoites. Sexual reproduction occurs in the mosquito, where new spores (sporozoites) are formed. Plasmodium knowlesi causes malaria, at least in some parts of Asia. In addition to mosquito bites and blood-contaminate needles, blood transfusion is a potentially important mode of transmission, at least in parts of the world in which screening of bank blood may not be as assiduous as it is in the United States.
1. Pathology and clinical significance:
Plasmodium sporozoites are injected into the bloodstream, where they rapidly migrate to the liver. There they form cyst-like structures containing thousands of merozoites. Upon release, the merozoites invade RBCs, using hemoglobin as a nutrient. Eventually, the infected RBCs rupture, releasing merozoites that can invade other erythrocytes. If large numbers of RBCs rupture at roughly the same time, a paroxysm (sudden onset) of fever can result from the massive release of toxic substances. A predictable consequence of RBC lysis is anemia, which is typical of Plasmodium infections. P. falciparum is the most dangerous plasmodial species. It can cause a rapidly fulminating disease, characterized by persistent high fever and ortho static hypotension. Infection can lead to capillary obstruction and death if treatment is not prompt. P. malariae, P. vivax, and P. ovale cause milder forms of the disease, probably because they invade either young or old red cells, but not both. This is in contrast to P. falciparum, which invades cells of all ages. Even today, malarial infection is a common and serious disease and in 2010 is estimated to have caused about 655,000 deaths worldwide. A summary of the life cycle of Plasmodium is shown in Figure 1.
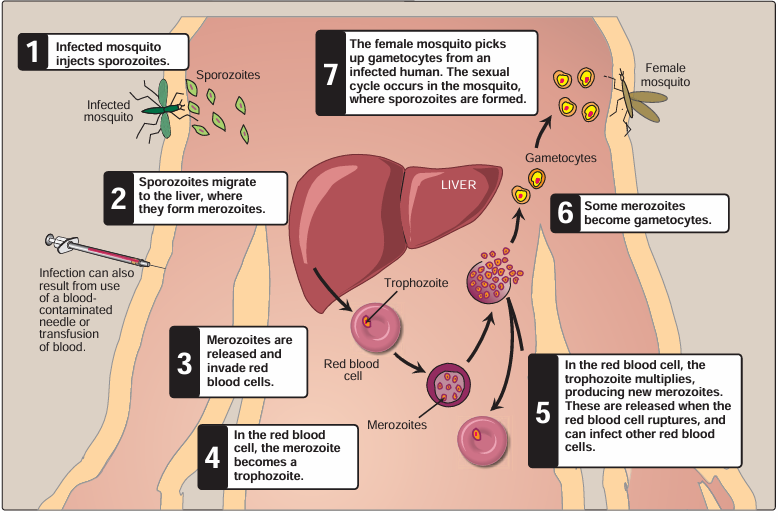
Fig1. Life cycle of the malarial parasite, Plasmodium falciparum.
2- Diagnosis and treatment:
Diagnosis depends on detection of the parasite inside RBCs (Figure 2). Thick blood smears stained with Giemsa stain provide the most sensitive visual test. Thin blood smears, in which more detail can be discerned, are used to determine the species involved, which is important in planning a course of therapy. Serologic tests are usually too slow for diagnosis of acute disease. Drug treatment is determined by the Plasmodium species that is causing the infection.
Because P. falciparum has no exoerythrocytic phase, it needs only to be treated with quinine, artemisin, mefloquine or doxycycline, depending on resistance patterns in the given geo graphic location. Chloroquine resistance is so prevalent among P. falciparum that it is almost never used for this organism any more. For ovale or vivax infections, after treatment with chloroquine, a two-week course of primaquine is necessary to achieve a “radical cure” by eliminating exoerythrocytic organ isms that persist in the liver. If, in the geographic location of infection, there is chloroquine resistance among P. vivax or P.ovale, then an alternative drug must be used prior to radical cure. Before treatment with primaquine, patients should be screened for glucose 6-phosphate dehydrogenase deficiency as individuals with deficiency of this enzyme develop hemolytic anemia, sometimes very severe, when treated with primaquine.
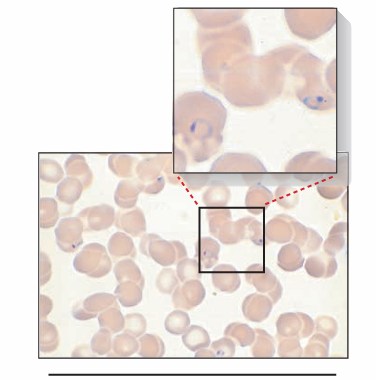
Fig2. Ring form of Plasmodium falciparum in red blood cell.





















