























النبات

مواضيع عامة في علم النبات
الجذور - السيقان - الأوراق
النباتات الوعائية واللاوعائية
البذور (مغطاة البذور - عاريات البذور)
الطحالب
النباتات الطبية
الحيوان
مواضيع عامة في علم الحيوان
علم التشريح
التنوع الإحيائي
البايلوجيا الخلوية
الأحياء المجهرية
البكتيريا
الفطريات
الطفيليات
الفايروسات
علم الأمراض
الاورام
الامراض الوراثية
الامراض المناعية
الامراض المدارية
اضطرابات الدورة الدموية
مواضيع عامة في علم الامراض
الحشرات
التقانة الإحيائية
مواضيع عامة في التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحيوية والميكروبات
الفعاليات الحيوية
وراثة الاحياء المجهرية
تصنيف الاحياء المجهرية
الاحياء المجهرية في الطبيعة
أيض الاجهاد
التقنية الحيوية والبيئة
التقنية الحيوية والطب
التقنية الحيوية والزراعة
التقنية الحيوية والصناعة
التقنية الحيوية والطاقة
البحار والطحالب الصغيرة
عزل البروتين
هندسة الجينات
التقنية الحياتية النانوية
مفاهيم التقنية الحيوية النانوية
التراكيب النانوية والمجاهر المستخدمة في رؤيتها
تصنيع وتخليق المواد النانوية
تطبيقات التقنية النانوية والحيوية النانوية
الرقائق والمتحسسات الحيوية
المصفوفات المجهرية وحاسوب الدنا
اللقاحات
البيئة والتلوث
علم الأجنة
اعضاء التكاثر وتشكل الاعراس
الاخصاب
التشطر
العصيبة وتشكل الجسيدات
تشكل اللواحق الجنينية
تكون المعيدة وظهور الطبقات الجنينية
مقدمة لعلم الاجنة
الأحياء الجزيئي
مواضيع عامة في الاحياء الجزيئي
علم وظائف الأعضاء
الغدد
مواضيع عامة في الغدد
الغدد الصم و هرموناتها
الجسم تحت السريري
الغدة النخامية
الغدة الكظرية
الغدة التناسلية
الغدة الدرقية والجار الدرقية
الغدة البنكرياسية
الغدة الصنوبرية
مواضيع عامة في علم وظائف الاعضاء
الخلية الحيوانية
الجهاز العصبي
أعضاء الحس
الجهاز العضلي
السوائل الجسمية
الجهاز الدوري والليمف
الجهاز التنفسي
الجهاز الهضمي
الجهاز البولي
المضادات الميكروبية
مواضيع عامة في المضادات الميكروبية
مضادات البكتيريا
مضادات الفطريات
مضادات الطفيليات
مضادات الفايروسات
علم الخلية
الوراثة
الأحياء العامة
المناعة
التحليلات المرضية
الكيمياء الحيوية
مواضيع متنوعة أخرى
الانزيمات

Streptococcus pneumoniae
 المؤلف:
Warren Levinson
المؤلف:
Warren Levinson
 المصدر:
Review of Medical Microbiology and Immunology
المصدر:
Review of Medical Microbiology and Immunology
 الجزء والصفحة:
13th Edition , p278-281
الجزء والصفحة:
13th Edition , p278-281
 2024-12-26
2024-12-26
 1249
1249




+
-
20
Diseases
Streptococcus pneumoniae causes pneumonia, bacteremia, meningitis, and infections of the upper respiratory tract such as otitis media, mastoiditis, and sinusitis. Pneumococci are the most common cause of community-acquired pneumonia, meningitis, sepsis in splenectomized individuals, otitis media, and sinusitis. They are a common cause of conjunctivitis, especially in children. Note that S. pneumoniae is also known as the pneumococcus (plural, pneumococci).
Important Properties
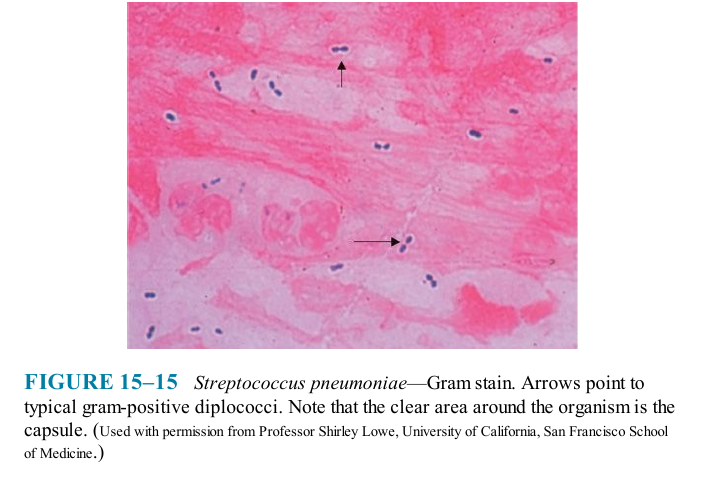
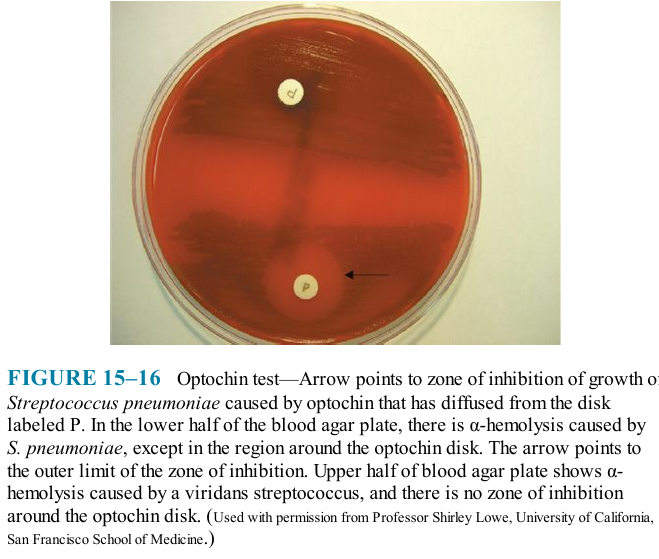
Pneumococci are gram-positive lancet-shaped cocci arranged in pairs (diplococci) or short chains (Figure 15-15). (The term lancet-shaped means that the diplococci are oval with somewhat pointed ends rather than being round.) On blood agar, they produce α-hemolysis. In contrast to viridans streptococci, they are lysed by bile or deoxycholate, and their growth is inhibited by optochin (Figure 15-16).
Pneumococci possess polysaccharide capsules of more than 85 antigenically distinct types. With type-specific antiserum, capsules swell (quellung reaction), and this can be used to identify the type. Capsules are virulence factors (i.e., they interfere with phagocytosis and favor invasiveness). Specific antibody to the capsule opsonizes the organism, facilitates phagocytosis, and promotes resistance. Such antibody develops in humans as a result either of infection (asymptomatic or clinical) or of administration of polysaccharide vaccine. Capsular polysaccharide elicits primarily a B-cell (i.e., T-independent) response.
Another important surface component of S. pneumoniae is a teichoic acid in the cell wall called C-substance (also known as C-polysaccharide). It is medically important not for itself, but because it reacts with a normal serum protein made by the liver called C-reactive protein (CRP). CRP is an “acute-phase" protein that is elevated as much as 1000-fold in acute inflammation. CRP is not an antibody (which are ϒ -globulins) but rather a β-globulin. (Plasma contains α-, β-, and ϒ -globulins.)
Note that CRP is a nonspecific indicator of inflammation and is elevated in response to the presence of many organisms, not just S. pneumoniae. Clinically, CRP in human serum is measured in the laboratory by its reaction with the carbohydrate of S. pneumoniae. The medical importance of CRP is that an elevated CRP appears to be a better predictor of heart attack risk than an elevated cholesterol level.
Transmission
Humans are the natural hosts for pneumococci; there is no animal reservoir. Because a proportion (5%-50%) of the healthy population harbors virulent organisms in the oropharynx, pneumococcal infections are not considered to be communicable. Resistance is high in healthy young people, and disease results most often when predisposing factors are present.
Pathogenesis
The most important virulence factor is the capsular polysaccharide, and anticapsular antibody is protective. Lipoteichoic acid, which activates complement and induces inflammatory cytokine production, contributes to the inflammatory response and to the septic shock syndrome that occurs in some immunocompromised patients. Pneumolysin, the hemolysin that causes α-hemolysis, may also contribute to pathogenesis.
Pneumococci produce IgA protease that enhances the organism's ability to colonize the mucosa of the upper respiratory tract. Pneumococci multiply in tissues and cause inflammation. When they reach alveoli, there is outpouring of fluid and red and white blood cells, resulting in consolidation of the lung. During recovery, pneumococci are phagocytized, mononuclear cells ingest debris, and the consolidation resolves.
Factors that lower resistance and predispose persons to pneumococcal infection include (1) alcohol or drug intoxication or other cerebral impairment that can depress the cough reflex and increase aspiration of secretions; (2) abnormality of the respiratory tract (e.g., viral infections), pooling of mucus, bronchial obstruction, and respiratory tract injury caused by irritants (which disturb the integrity and movement of the mucociliary blanket); (3) abnormal circulatory dynamics (e.g., pulmonary congestion and heart failure); (4) splenectomy; and (5) certain chronic diseases such as sickle cell anemia and nephrosis. Patients with sickle cell anemia auto- infarct their spleen, become functionally asplenic, and are predisposed to
pneumococcal sepsis. Trauma to the head that causes leakage of spinal fluid through the nose predisposes to pneumococcal meningitis.
 الاكثر قراءة في البكتيريا
الاكثر قراءة في البكتيريا
 اخر الاخبار
اخر الاخبار
اخبار العتبة العباسية المقدسة

الآخبار الصحية


مواضيع ذات صلة
 قسم الشؤون الفكرية يصدر كتاباً يوثق تاريخ السدانة في العتبة العباسية المقدسة
قسم الشؤون الفكرية يصدر كتاباً يوثق تاريخ السدانة في العتبة العباسية المقدسة "المهمة".. إصدار قصصي يوثّق القصص الفائزة في مسابقة فتوى الدفاع المقدسة للقصة القصيرة
"المهمة".. إصدار قصصي يوثّق القصص الفائزة في مسابقة فتوى الدفاع المقدسة للقصة القصيرة (نوافذ).. إصدار أدبي يوثق القصص الفائزة في مسابقة الإمام العسكري (عليه السلام)
(نوافذ).. إصدار أدبي يوثق القصص الفائزة في مسابقة الإمام العسكري (عليه السلام)



















