























النبات

مواضيع عامة في علم النبات
الجذور - السيقان - الأوراق
النباتات الوعائية واللاوعائية
البذور (مغطاة البذور - عاريات البذور)
الطحالب
النباتات الطبية
الحيوان
مواضيع عامة في علم الحيوان
علم التشريح
التنوع الإحيائي
البايلوجيا الخلوية
الأحياء المجهرية
البكتيريا
الفطريات
الطفيليات
الفايروسات
علم الأمراض
الاورام
الامراض الوراثية
الامراض المناعية
الامراض المدارية
اضطرابات الدورة الدموية
مواضيع عامة في علم الامراض
الحشرات
التقانة الإحيائية
مواضيع عامة في التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحيوية والميكروبات
الفعاليات الحيوية
وراثة الاحياء المجهرية
تصنيف الاحياء المجهرية
الاحياء المجهرية في الطبيعة
أيض الاجهاد
التقنية الحيوية والبيئة
التقنية الحيوية والطب
التقنية الحيوية والزراعة
التقنية الحيوية والصناعة
التقنية الحيوية والطاقة
البحار والطحالب الصغيرة
عزل البروتين
هندسة الجينات
التقنية الحياتية النانوية
مفاهيم التقنية الحيوية النانوية
التراكيب النانوية والمجاهر المستخدمة في رؤيتها
تصنيع وتخليق المواد النانوية
تطبيقات التقنية النانوية والحيوية النانوية
الرقائق والمتحسسات الحيوية
المصفوفات المجهرية وحاسوب الدنا
اللقاحات
البيئة والتلوث
علم الأجنة
اعضاء التكاثر وتشكل الاعراس
الاخصاب
التشطر
العصيبة وتشكل الجسيدات
تشكل اللواحق الجنينية
تكون المعيدة وظهور الطبقات الجنينية
مقدمة لعلم الاجنة
الأحياء الجزيئي
مواضيع عامة في الاحياء الجزيئي
علم وظائف الأعضاء
الغدد
مواضيع عامة في الغدد
الغدد الصم و هرموناتها
الجسم تحت السريري
الغدة النخامية
الغدة الكظرية
الغدة التناسلية
الغدة الدرقية والجار الدرقية
الغدة البنكرياسية
الغدة الصنوبرية
مواضيع عامة في علم وظائف الاعضاء
الخلية الحيوانية
الجهاز العصبي
أعضاء الحس
الجهاز العضلي
السوائل الجسمية
الجهاز الدوري والليمف
الجهاز التنفسي
الجهاز الهضمي
الجهاز البولي
المضادات الميكروبية
مواضيع عامة في المضادات الميكروبية
مضادات البكتيريا
مضادات الفطريات
مضادات الطفيليات
مضادات الفايروسات
علم الخلية
الوراثة
الأحياء العامة
المناعة
التحليلات المرضية
الكيمياء الحيوية
مواضيع متنوعة أخرى
الانزيمات

Laboratory and Diagnostic Testing
 المؤلف:
المرجع الالكتروني للمعلوماتية
المؤلف:
المرجع الالكتروني للمعلوماتية
 المصدر:
almerja.com
المصدر:
almerja.com
 الجزء والصفحة:
الجزء والصفحة:
 15-2-2016
15-2-2016
 2507
2507




+
-
20
Laboratory and Diagnostic Testing
Laboratory and diagnostic tests are tools to gain additional information about the patient. By themselves, these tests are not therapeutic; however, when used in conjunction with a thorough history and physical examination, these tests may confirm a diagnosis or provide valuable information about a patient's status and response to therapy that may not be apparent from the history and physical examination alone.
Generally, an evidenced-based tiered approach to selecting tests is used:
-Basic screening (frequently used with wellness groups and case finding)
-Establishing (initial) diagnoses
-Differential diagnosis
-Evaluating current medical case management and outcomes
-Evaluating disease severity
-Monitoring course of illness and response to treatment
-Group and panel testing
-Regularly scheduled screening tests as part of ongoing care
-Testing related to specific events, certain signs and symptoms, or other exceptional situations (eg, infection and inflammation [bladder infection or cellulitis], sexual assault, drug screening, pheochromocytoma, postmortem tests, to name a few) .
Test selections are based on subjective clinical judgment, national recommendations, and evidence-based health care. Often diagnostic tests or procedures are used as predictors of surgical risk or morbidity and mortality rates because, in some cases, the risk may outweigh the benefit. The clinician’s main task is to make reasoned decisions about patient care despite incomplete clinical information and uncertainty about clinical outcomes. While data elicited from the history and physical examination are often sufficient for making a diagnosis or for guiding therapy, more information may be required. In these situations, clinicians often turn to diagnostic tests for help.
BENEFITS; COSTS, AND RISKS
When used appropriately, diagnostic tests can be of great assistance to the clinician. Tests can be helpful for screening, ie, to identify risk factors for disease and to detect occult disease in asymptomatic persons. Identification of risk factors may allow early intervention to prevent disease occurrence, and early detection of occult disease may reduce disease morbidity and mortality through early treatment. Some tests assist in early diagnosis after onset of symptoms and signs; others assist in differential diagnosis of various possible diseases; others help determine the stage or activity of disease. Finally, tests can be helpful in patient management. Tests can help:
- evaluate the severity of disease.
- estimate prognosis.
- monitor the course of disease (progression, stability, or resolution).
- detect disease recurrence, and select drugs and adjust therapy.
When ordering diagnostic tests, clinicians should weigh the potential benefits against the potential costs and disadvantages:
- Some tests carry a risk of morbidity or mortality—eg, cerebral angiogram leads to stroke in 1% of cases.
- The discomfort associated with tests such as sigmoidoscopy or barium enema will deter some patients from completing a diagnostic work-up.
- The result of a diagnostic test often has implications for further care in that a test result may mandate further testing or frequent follow-up. This means that a patient with a positive fecal occult blood test may incur significant cost, risk, and discomfort during follow-up sigmoidoscopy, barium enema, or colonoscopy.
- A false-positive test may lead to further unnecessary testing. Classifying a healthy patient as diseased based on a falsely positive diagnostic test can cause psychologic distress and may lead to risks from unnecessary therapy.
- A diagnostic or screening test may identify cases of disease that would not otherwise have been recognized and that would not have affected the patient. For example, early-stage, low-grade prostate cancer detected by PSA screening in an 84-year-old man with known severe congestive heart failure will probably not become symptomatic or require treatment during his lifetime.
- An individual test such as MRI of the head can cost more than $1400, and diagnostic tests as a whole account for approximately one-fifth of health care expenditures in the USA.
CRITERIA FOR USE OF SCREENING PROCEDURES.
A- Characteristics of population
- Sufficiently high prevalence of disease.
- Likely to be compliant with subsequent tests and treatments.
B- Characteristics of disease
- Significant morbidity and mortality.
- Effective and acceptable treatment available.
- Pre-symptomatic period detectable.
- Improved outcome from early treatment.
C- Characteristics of test
- Good sensitivity and specificity.
- Low cost and risk.
- Confirmatory test available and practical.
TEST CHARACTERISTICS Accuracy
The accuracy of a laboratory test is its correspondence with the true value. In the clinical laboratory, accuracy of tests is maximized by calibrating laboratory equipment with reference material and by participation in external quality control programs.
Precision
Test precision is a measure of a test’s reproducibility when repeated on the same sample. An imprecise test is one that yields widely varying results on repeated measurements . The precision of diagnostic tests, which is monitored in clinical laboratories by using control material, must be good enough to distinguish clinically relevant changes in a patient’s status from the analytic variability of the test. For instance, the manual white blood cell differential count is not precise enough to detect important changes in the distribution of cell types, because it is calculated by subjective evaluation of a small sample (100 cells). Repeated measurements by different technicians on the same sample result in widely different results. Automated differential counts are more precise because they are obtained from machines that use objective physical characteristics to classify a much larger sample (10,000 cells).
PROPERTIES OF USEFUL DIAGNOSTIC TESTS.
- Test methodology has been described in detail so that it can be accurately and reliably reproduced.
- Test accuracy and precision have been determined.
- The reference range has been established appropriately.
- Sensitivity and specificity have been reliably established by comparison with a gold standard. The evaluation has used a range of patients, including those who have different but commonly confused disorders and those with a spectrum of mild and severe, treated and untreated disease. The patient selection process has been adequately described so that results will not be generalized inappropriately.
Independent contribution to overall performance of a test panel has been confirmed if a test is advocated as part of a panel of tests.
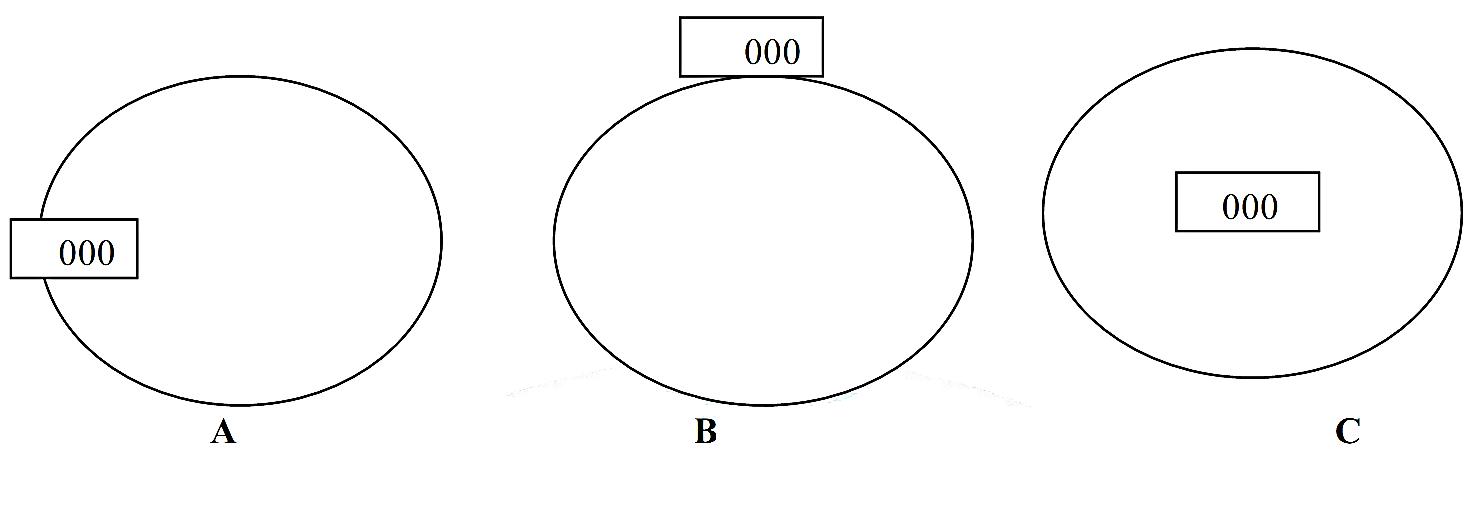
Figure 1 Relationship between accuracy and precision in diagnostic tests. The center of the target represents the true value of the substance being tested. Figure (A) represents a diagnostic test which is precise but inaccurate; on repeated measurement, the test yields very similar results, but all results are far from the true value. Figure (B) shows a test which is imprecise and inaccurate; repeated measurement yields widely different results, and the results are far from the true value. Figure (C) shows an ideal test, one that is both precise and accurate.
Reference Range
Reference ranges are method- and laboratory-specific. In practice, they often represent test results found in 95% of a small population presumed to be healthy; by definition, then, 5% of healthy patients will have a positive (abnormal) test. As a result, slightly abnormal results should be interpreted critically— they may be either truly abnormal or falsely abnormal. It is important to consider also whether published reference ranges are appropriate for the patient being evaluated, since some ranges depend on age, sex, weight, diet, time of day, activity status, or posture. For instance, the reference ranges for hemoglobin concentration are age- and sex-dependent.
Interfering Factors
The results of diagnostic tests can be altered by external factors, such as ingestion of drugs; and internal factors, such as abnormal physiologic states. External interferences can affect test results in vivo or in vitro. In vivo, alcohol increases glutamyl transpeptidase, and diuretics can affect sodium and potassium concentrations. Cigarette smoking can induce hepatic enzymes and thus reduce levels of substances such as theophylline that are metabolized by the liver. As an example, patients with gross lipemia may have spuriously low serum sodium levels if the test methodology used includes a step in which serum is diluted before sodium is measured. Because of the potential for test interference, clinicians should be wary of unexpected test results and should investigate reasons other than disease that may explain abnormal results, including laboratory error.
Sensitivity and Specificity
Clinicians should use measures of test performance such as sensitivity and specificity to judge the quality of a diagnostic test for a particular disease. Test sensitivity is the likelihood that a diseased patient has a positive test. If all patients with a given disease have a positive test (i.e., no diseased patients have negative tests), the test sensitivity is 100%. A test with high sensitivity is useful to exclude a diagnosis because a highly sensitive test will render few results that are falsely negative. To exclude infection with the AIDS virus, for instance, a clinician might choose a highly sensitive test such as the HIV antibody test.
A test’s specificity is the likelihood that a healthy patient has a negative test. If all patients who do not have a given disease have negative tests (i.e., no healthy patients have positive tests), the test specificity is 100%. A test with high specificity is useful to confirm a diagnosis, because a highly specific test will have few results that are falsely positive. For instance, to make the diagnosis of gouty arthritis, a clinician might choose a highly specific test, such as the presence of negatively birefringent needle shaped crystals within leukocytes on microscopic evaluation of joint fluid. To determine test sensitivity and specificity for a particular disease, the test must be compared against a “gold standard,” a procedure that defines the true disease state of the patient.
 الاكثر قراءة في التحليلات المرضية
الاكثر قراءة في التحليلات المرضية
 اخر الاخبار
اخر الاخبار
اخبار العتبة العباسية المقدسة

الآخبار الصحية


مواضيع ذات صلة
 قسم الشؤون الفكرية يصدر كتاباً يوثق تاريخ السدانة في العتبة العباسية المقدسة
قسم الشؤون الفكرية يصدر كتاباً يوثق تاريخ السدانة في العتبة العباسية المقدسة "المهمة".. إصدار قصصي يوثّق القصص الفائزة في مسابقة فتوى الدفاع المقدسة للقصة القصيرة
"المهمة".. إصدار قصصي يوثّق القصص الفائزة في مسابقة فتوى الدفاع المقدسة للقصة القصيرة (نوافذ).. إصدار أدبي يوثق القصص الفائزة في مسابقة الإمام العسكري (عليه السلام)
(نوافذ).. إصدار أدبي يوثق القصص الفائزة في مسابقة الإمام العسكري (عليه السلام)



















