
Oesophagitis
 المؤلف:
James Carton
المؤلف:
James Carton
 المصدر:
Oxford Handbook of Clinical Pathology 2024
المصدر:
Oxford Handbook of Clinical Pathology 2024
 الجزء والصفحة:
3rd edition , p110-111
الجزء والصفحة:
3rd edition , p110-111
 2025-02-01
2025-02-01
 770
770
Definition
• Inflammation of the oesophagus.
Presentation
• Burning retrosternal pain (heartburn).
• Dysphagia and hiccups may also occur.
Reflux oesophagitis
• Caused by gastric acid refluxing into the lower oesophagus.
• Very common. Most prevalent in adult white males but can occur in men and women of all races and in children.
• Predisposing conditions include obesity, alcohol, medications, hypothyroidism, pregnancy, hiatus hernia, and diabetes.
• Mucosal biopsy shows regenerative changes of the squamous epithelium demonstrated by basal cell hyperplasia and extension of vascular papillae into the upper part of the epithelium. Spongiosis (intercellular oedema) is a characteristic feature. Inflammation is typically mild with scattered neutrophils and eosinophils.
• ~10% of patients develop columnar metaplasia of the lower oesophagus which is visible endoscopically; this is known as Barrett’s oesophagus or columnar-lined oesophagus (fig.1). there may also be intestinal metaplasia with goblet cells. this is associated with a higher risk of developing oesophageal adenocarcinoma. It should be noted that in the USA goblet cells are essential to make the diagnosis.
- Barrett’s oesophagus is associated with a 50 times increased risk of oesophageal adenocarcinoma. Patients with Barrett’s oesophagus should be considered for entry into a surveillance programme of regular endoscopy and biopsy to check for columnar epithelial dysplasia. Dysplasia is divided into high grade and low grade. this is a subjective assessment and current national guidelines state that it should always be made by two pathologists.
Drug- induced (‘pill’) oesophagitis
• Caused by direct toxicity of drugs to the oesophageal mucosa.
• Occurs mostly in the elderly.
• Common culprit drugs are bisphosphonates and iron tablets.
• Mucosal biopsy shows acute inflammation with erosion or ulceration of the surface epithelium. encrusted golden brown iron pigment may be seen in cases caused by iron tablets.
• Usually resolves after discontinuation of the offending drug.
Eosinophilic oesophagitis
• Uncommon condition which occurs mostly in atopic individuals with a history of allergy, asthma, and drug sensitivities.
• Mucosal biopsy shows heavy infiltration of the mucosa by eosinophils (more than 15/ high- powered field) which often form clusters (‘micro- abscesses’). Note that smaller numbers of eosinophils are common in reflux oesophagitis. for this reason, it is helpful to take biopsies from all levels of the oesophagus.
• May coexist with reflux oesophagitis.
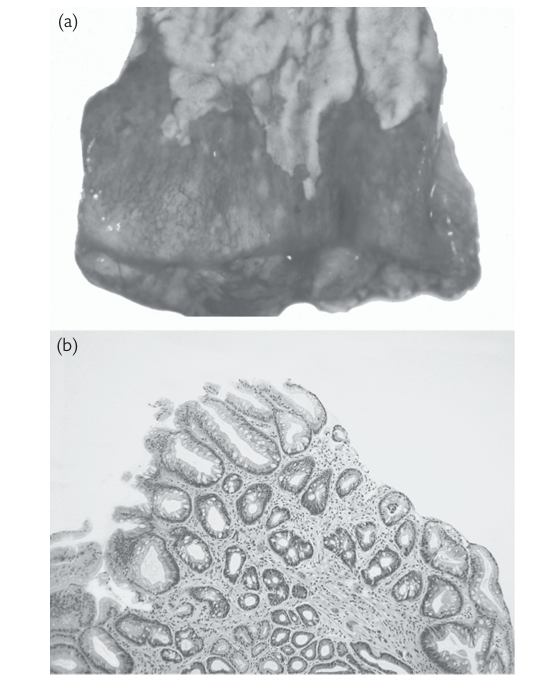
fig1. Barrett’s oesophagus. (a) this segment from the lower oesophagus shows the white keratinized squamous epithelium at the top. the red area at the bottom represents an area of Barrett’s oesophagus. (b) An oesophageal biopsy taken from an area of endoscopic Barrett’s oesophagus, confirming the presence of glandular epithelium (see Plate 9). reproduced with permission from Clinical Pathology (Oxford Core texts), Carton, James, Daly, richard, and ramani, Pramila, Oxford University Press (2006), p.139, figure 8.1.
• Good outlook if diagnosed and treated early. If untreated, it can lead to severe oesophageal strictures.
Infectious oesophagitis
• More commonly seen in debilitated or immunocompromised patients, as the oesophagus is normally highly resistant to infection.
• Common infectious agents include herpes simplex virus (HSV), cytomegalovirus (CMV), and Candida
 الاكثر قراءة في مواضيع عامة في علم الامراض
الاكثر قراءة في مواضيع عامة في علم الامراض
 اخر الاخبار
اخر الاخبار
اخبار العتبة العباسية المقدسة




















